Available online on www.ijppr.com International Journal of Pharmacognosy and Phytochemical Research 2012-13; 4(4); 213-218
ISSN: 0975-4873 Author for correspondence: E-mail: rohit.gundamaraju@gmail.com
Research Article Evaluation of Anti-Obesity Activity of Lantana camara Var Linn. by Progesterone Induced Obesity on Albino Mice *1Rohit Gundamaraju, 1Sartaj Banu Mulaplli, 2Dr.Ramesh.C. Department of Pharmacolgy , Malla Reddy Institute of Pharmaceutical Sciences , Maisammagud , Dhulapally(Post via Hakimpet) ,Secunderabad (500014), AP,India. 2 GSN Pharmaceuticals Pvt .Ltd., Rajeev Gandhi Nagar, Kukatpally, Hyderabad (500072),AP,India. ABSTRACT The anti-obesic activity of Lantana camara was studied on progesterone induced models of hyperlipedemia in mice. Hyperlipidemia condition established by progesterone, which changed various parameters in the body . An increase in food consumption and water consumption usually accompanies the body weight gain, which is the characteristic nature of progesterone stimulation. Increased consumption of food and water generally leads to elevated parameters like LDL,VLDL, serum cholesterol etc. Accumulation of fat in areas like inguinal, epididymal , neck etc. was observed . Ethanobotanical knowledge of medicinal plants is one of the most prominent source of new drugs and has shown potential results for treatment of obesity. Preliminary phytochemical analysis of Lantana camara revealed the presence of phyto constituents such as steroids , flavinoids , alkaloids, etc. Keywords: Adipocyte, progesterone, Obesity INTRODUCTION Obesity is a chronic metabolic disorder caused by an imbalance between energy intake and expenditure. Over weight and obesity are defined as abnormal or excessive fat accumulation that presents a risk to health. Obesity is one of the greatest health threats of this century. Chronic obesity is a problem of epidemic proportions, and is rapidly increasing in prevalence in both the West and the Asia-Pacific region¹ ˉ² which has an important impact on life style-related diseases such as coronary heart disease, dyslipidemia, glucose intolerance, diabetics, hypertension and some cancers³ . Several factors, including lack of exercise, sedentary lifestyles and the consumption of energy rich diets are contributory to the etiology of obesity⁴. Despite the urgent need for safe and efficient therapeutics and the potential size of the market for anti-obesity drugs, the current status for the development of such drugs are still unsatisfactory ⁵. Some edible medicinal plants have been used as dietary supplements for body-weight management and control in many countries⁶ˉ⁷ . In the literature survey, it was found that flavonoids, sterols, tannins, and alkaloids have shown promising effects to tackle obesity by various mechanisms, Lantana camara whole plant has shown the presence of sterols, triterpenoids, flavonoids alkaloids and saponins, and others in the extracts. Moreover, traditional Indian medicine also claims for its antiobesity activity. With this back ground, this plant has been selected for its phytochemical analysis and screening of its antiobesity activity against progesterone-induced obesity in female mice. The neuroactive steroid, progesterone is a female reproductive hormone. Its level increases during the later phase of the menstrual cycle and controls the secretory phase of the endometrium. Substantial evidence links progesterone excess in pathophysiology of eating and affective disorders. Some reports suggest the use of progesterone-containing preparations as contraceptive or for the hormone replacement therapy to cause sufficient weight gain by causing hyperphagia and increased fat deposition in the body⁸. Reports also suggest that progesterone can produce these effects by inducing myriad of neurotransmitter changes of which alterations of serotonin level can have important. With this setting neuroactive to induce obesity in female mice has been chosen. MATERIALS AND METHODS Collection of plant material: Lantana camara whole plants materials were collected from Tirupathi . The plant authentication was done by Department of Botany,Sri Venkateshwara University , Tirupathi dist. Chittoor , Andhra Pradesh, and the voucher was preserved.
Preparation of the extract: Leaves of Lantana camara were shade dried at room temperature for 2-3 days. These dried leaves were then powdered in a mixture. The extraction process was done in a Soxhlet extractor. The fine powder (100 grams ) was suspended in (200 ml) of methanol for 24 hours at room temperature. After extraction , the solvent was evaporated by rotary evaporator and the residue was dried.⁹ Experimental animals: Female albino mice (20–25 g) were used in this study. Mice bred at GSN Pharmaceuticals PVT.LTD animal house were used in this experiment. Animals were housed in a standard controlled animal care facility in cages (5 mice/cage). Rohit Gundamaraju et,al./ Evaluation of Anti-Obesity… IJPPR, Vol-4, Issue 4, December 2012- February 2013, 213-218
Page214 The following table consists of the data derived from the results of the histopathology of the various slides consisting of the organs(liver) sections of various groups. The table consists of the inducing agent, size of the organs, changes observed, and conclusions drawn.
S.NO
GROUP
SIZE
COLOR
INFERENCE
CONCLUSION
1.
INDUCING AGENT
Slight increase
normal
Mild fatty change
The liver is prone to fatty diet,as there is increase in the fat cells.
2.
INDUCING AGENT + TREATED DRUG EXTRACT
normal
normal
Positive necrosis,focal necrosis of hepatocytes,swelling found
Extract found to show effect on liver.fatty change is abscent ,drug extract found to show its action on the fatty liver.
3.
INDUCING AGENT + TREATED DRUG EXTRACT(DOUBLE DOSE)
normal
normal
Focal necrosis,swelling of hepatocytes with change in the cells and degenation in some places,
Extract found to show its action on liver,fatty change is abscent,drug extract found to show its action on the fatty liver
4.
INDUCING AGENT + STANDARD DRUG
normal
normal
Mild necrosis found. Less extent when compared to 2nd and 3rd conditions.
First of all, I want to put front a statement that ageing and process of ageing will be a very challenging part in research which would be very synergic aspect in research on diseases, and common disorders like erectile dysfunction.
Nitric oxide and aging of LHRH and oxytocin systems
While the involvement of NO in hypothalamic regulation of LHRH and oxytocin release is becoming accepted, the putative role of NO as a potential proapoptotic factor for LHRH and oxytocin neurons has not been extensively studied until recently. Vernet et al. suggested that increased expression of iNOS may lead to neurotoxicity, which can be involved in impaired pulsatile LHRH secretion, as well as acts as a possible inducer of age-associated neuronal loss. Recent findings of aging-related iNOS induction in LHRH and oxytocinergic neurons support the view that iNOS expression is associated with the previously observed decrease in the number of LHRH] and oxytocin cells. This suggests an additional, possibly destructive action of NO on the hypothalamic neuroendocrine pathways. The endogenous factors that induce iNOS expression in aging LHRH and oxytocinergic hypothalamic neurons are unknown. Nevertheless, indirect observations seem to indicate cytokines as potential regulators of the age-related iNOS induction. Earlier studies revealed that TNF-γ in the cerebrospinal fluid and peripheral circulation and IL-1β and interferon-γ were increased in monocytes by aging. Cytokines were found to be synthesized in the hypothalamus. Accordingly, observation that the exogenous administration of interleukin 1-α can block the nitrergic control of LHRH release both in vivo and in vitro through iNOS induction, additionally implicates cytokines in aging-related control of iNOS expression in the hypothalamic neurons.
Bacterial and viral products, such as bacterial lipopolysaccharide (LPS), cause inducible (i) NO synthase (NOS) synthesis, which in turn produces massive amounts of nitric oxide (NO). NO, by inactivating enzymes and leading to cell death, is toxic not only to invading viruses and bacteria, but also to host cells. Injection of LPS induces interleukin (IL)-1beta, IL-1alpha, and iNOS synthesis in the anterior pituitary and pineal glands, meninges, and choroid plexus, regions outside the blood-brain barrier. Thereafter, this induction occurs in the hypothalamic regions (such as the temperature-regulating centers), paraventricular nucleus (releasing and inhibiting hormone neurons), and the arcuate nucleus (a region containing these neurons and axons bound for the median eminence). Aging of the anterior pituitary and pineal with resultant decreased secretion of pituitary hormones and the pineal hormone melatonin, respectively, may be caused by NO. The induction of iNOS in the temperature-regulating centers by infections may cause the decreased febrile response in the aged by loss of thermosensitive neurons. NO may play a role in the progression of Alzheimer's disease and parkinsonism. LPS similarly activates cytokine and iNOS production in the cardiovascular system leading to coronary heart disease. Fat is a major source of NO stimulated by leptin. As fat stores increase, leptin and NO release increases in parallel in a circadian rhythm with maxima at night. NO could be responsible for increased coronary heart disease as obesity supervenes. Antioxidants, such as melatonin, vitamin C, and vitamin E, probably play important roles in reducing or eliminating the oxidant damage produced by NO.
Over the past ten years despite a slight increase in life expectancy and a decrease in all causes of deaths, the percent of the US population with heart disease, cancer, diabetes, hypertension and obesity have all increased. According to the 2010 National Center for Health Statistics Report life expectancy has increased 1.1 years over the past decade going from 76.8 to 77.9. All causes of death adjusted for age have decreased by 12.5% from 2000 to 2008. However, the percent of the population 18 years and over with heart disease has risen from 10.9% to 11.8% and the population 65 and over has risen from 29.6% to 31.7% over the same 8 years. Diabetes has gone from 8.5% of the population 20 years and older to 11.9% in just 8 years. The percent of people with hypertension has risen from 28.9% to 32.6%. Cancer has followed a similar trend going from 4.9% to 6.1% in patients 18 years old and over. These data suggests that although people are living longer, they are not living better or they are living with a chronic disease that requires care and treatment. It is the care and treatment of these chronic patients that causes the enormous economic burden on the health care system and on the patients. In fact from 2000 to 2008, total healthcare expenditures increased from $1.1 to $2.0 trillion dollars or from $4,032 to $6,411 per capita.
This trend is also reflective of the global population where 17.3 million people died from cardiovascular disease in 2008 and an estimated 23.6 million expect to die in 2030. Whereas access to medical care and better management of certain diseases have improved, it is clear that the incidence and treatment of chronic disease is not improving. The discovery of nitric oxide (NO) production in the human body is a relatively new advancement of modern medicine. Unfortunately is still not at the forefront of modern medicine. There are no standard laboratory measurements of NO in the clinical setting and no prescription therapies to safely and effectively restore NO homeostasis despite being recognized as the earliest indicator of a number of different chronic diseases. We also now know that modern medical practices and western lifestyles actually lead to a decrease in NO homeostasis in the patients from pediatrics to geriatrics.
The discovery of nitric oxide (NO) in the 1980s as a vasodilator and signaling molecule in the cardiovascular system, immune system and nervous system marked a point of inflexion in medicine. The discovery that a simple molecule produced as a gas could perform so many essential and critical biological and physiological functions established a new paradigm in cell signaling. Now almost 30 years later, endothelial dysfunction or insufficient NO production is recognized as the earliest event in the onset and progression of a number of chronic diseases. Loss of endothelial NO function is associated with several cardiovascular disorders, including atherosclerosis, which is due either to decreased production or to increased degradation of NO. A number of studies provide evidence that endothelial NO dysfunction is not only associated with all major cardiovascular risk factors, such as hyperlipidemia, diabetes, hypertension, smoking and severity of atherosclerosis, but also has a profound predictive value for the future atherosclerotic disease progression. There is becoming a clear and convincing association with Alzheimers disease (AD) and NO. Decreased levels of nitrite and nitrate (NOx) has been detected in patients with different forms of dementia especially AD. The exact etiology of sporadic AD is unclear, but it is interesting that cardiovascular risk factors including hypertension, hypercholesterolemia, diabetes mellitus, aging, and sedentary lifestyle are associated with higher incidence of AD (all conditions associated with NO insufficiency). The link between cardiovascular risk factors and AD has yet to be identified; however, a common feature is endothelial dysfunction, specifically, decreased bioavailability of NO. Insulin has vasodilator actions that depend on endothelium-derived NO. Type 2 diabetes mellitus accounts for 80-90% of diabetes cases in the US and is associated with an increased risk for a number of life-threatening complications. These include heart disease and stroke, high blood pressure, blindness, kidney disease, nervous system disease, amputation, and complications of pregnancy and surgery. Probably not coincidental, all of the above complications are associated with insufficient NO production. Endothelial dysfunction with reduced NO generation and bioavailability plays a key role in the pathogenesis of diabetic vascular disease and complications and likely serves as the key link between metabolic disorders and cardiovascular disease (CVD).
While the medical literature is rich with clear association and almost causal relationships between NO and the onset and progression of chronic disease, it is not commonly considered in the treatment or management of patients. In fact, some prescription medications will reduce NO availability, many lifestyle and dietary habits that lead to chronic disease are linked to insufficient NO production or availability and the standard of care for patients in intensive care units or hemodialysis patients leads to a complete removal of NO functionality in the patients.
Despite NO being recognized by the scientific and medical community as one of the most important molecules produced within the body and being named “Molecule of the Year” by Science in 1992 and a Nobel Prize in Physiology or Medicine awarded for its discovery, there are currently only 3 FDA approved products on the market directly related to NO: 1) organic nitrates, such as nitroglycerin for the treatment of acute angina (these have been used for centuries long before the discovery of NO); 2) inhaled NO therapy for neonates for treatment of pulmonary hypertension due to underdeveloped lungs; and 3) phosphodiesterase inhibitors, such as sildenafil, which do not directly affect NO production but act through affecting the downstream second messenger of NO, cyclic guanosine monophosphate (cGMP). With the knowledge gained in the physiology and pharmacology of NO, better and new drugs are being designed not only for cardiovascular diseases but for neurological and several other disorders as well.
One of the most predictive indicators for insufficient NO production is age. As we age we lose our ability to produce NO through the L-arginine pathway. Aging and hypertension are well-documented cardiovascular risk factors. Most of the functional and structural vascular alterations that lead to cardiovascular complications are similar in aging and hypertension [20]. Moreover, these vascular changes associated with essential hypertension are generally considered to be an accelerated form of the changes seen with aging. When we are young and healthy, the endothelial production of NO through L-arginine is efficient and sufficient to produce NO; however, as we age we lose our ability to synthesize endothelial derived NO. Most of the works on the activity of NO in cells and tissues agree that the bioavailability or the generation of NO decreases with aging. It has been proposed that superoxide can scavenge NO to form peroxynitrite and thereby reduce its effective concentrations in cells. It has also been reported that there is decreased nitric oxide synthase (NOS) expression with aging both in constitutive and inducible isoforms. Berkowitz et al. observed the upregulation of arginase (an enzyme that degrades the natural substrate for NOS, L-arginine) in aged blood vessels and the corresponding modulation of NOS activity. Taddei et al. have shown that there is a gradual decline in endothelial function due to aging with greater than 50% loss in endothelial function in the oldest age group tested as measured by forearm blood flow assays. Egashira et al. reported more dramatic findings in the coronary circulation of aging adults whereby there was a loss of 75% of endothelium-derived nitric oxide in 70-80 year old patients compared to young, healthy 20 year olds. Vita and colleagues demonstrated that increasing age was one predictor of abnormal endothelium-dependent vasodilation in atherosclerotic human epicardial coronary arteries. Gerhard et al., concluded from their 1996 study that age was the most significant predictor of endothelium-dependent vasodilator responses by multiple stepwise regression analysis. Collectively, these important findings illustrate that endothelium-dependent vasodilation in resistance vessels declines progressively with increasing age. This abnormality is present in healthy adults who have no other cardiovascular risk factors, such as diabetes, hypertension, or hypercholesterolemia. Most of these studies found that impairment of endothelium-dependent vasodilation was clearly evident by the fourth decade. In contrast, endothelium-independent vasodilation does not change significantly with aging, demonstrating that the responsiveness to NO does not change only the ability to generate it. These observations enable us to conclude that reduced availability of endothelium-derived NO occurs as we age. Being able to diagnose and intervene early on is the key to optimal health and disease prevention.
Mystery disease !!!! The name itself has the meaning,"mystery" that means neither any one does know the cause, nor even the name of the disease. Many diseases are throwing a challenge for researchers and doctors all around the world. Most of these diseases are so exotic and dangerous that we doesnt' even know the root cause. Such diseases when hit the humans, will cause a serious nebulic situation where we cant proceed with the treatment.
Can any one dare to imagine? , A small cute little girl who is always indulged in fun and laughter, who doesnt' know anything other than love and affection is now prone to such a condition where she has left nothning to her parents except agony.
Brianna Skriver was a bouncy, blond "wild child" who loved playing dress-up and jumping rope with her fellow 5-year-olds, according to her mom. But a mysterious illness swiftly stole her ability to walk and talk, leaving her family desperate for answers.
It all started at a soccer game.
"I noticed she was running differently and falling a lot," said Skriver's mom, Tammy Skriver, a single mother of two in Central Florida. "When we got home I said, 'Show mommy how you skip' -- she loved to skip -- and she couldn't do it."
Skriver became increasingly lethargic, and soon began drooling and wetting the bed. Within a year, she could no longer walk. And by age 9, she needed a feeding tube. But countless blood tests, biopsies, brain scans and spinal taps have failed to uncover the cause of her ever-worsening condition.
"Doctors say it's a neurodegenerative disorder, but they don't know what it is or why it's happening," said Tammy Skriver, talking through tears. "It's excruciating. I get down on my knees all the time and just pray this is a dream."
Now doctors arent' able to judge what is the root cause of this condition.
This is high-time for researchers to take a forward step in research and i strongly urge that governments all around the world should endorse the research firms and encourage in research.
Ebola virus disease (EVD) or Ebola hemorrhagic fever (EHF) is the human disease which may be caused by any of four of the five known ebola viruses. These four viruses are: Bundibugyo virus (BDBV), Ebola virus (EBOV), Sudan virus (SUDV), and Taï Forest virus (TAFV, formerly and more commonly Côte d'Ivoire Ebola virus (Ivory Coast Ebolavirus, CIEBOV)). EVD is a viral hemorrhagic fever (VHF), and is clinically nearly indistinguishable from Marburg virus disease (MVD).
Symptoms :
EVD/EHF is clinically indistinguishable from Marburg virus disease (MVD), and it can also easily be confused with many other diseases prevalent in Equatorial Africa, such as other viral hemorrhagic fevers, falciparum malaria, typhoid fever, shigellosis, rickettsial diseases, cholera, gram-negative septicemia or EHEC enteritis. The most detailed studies on the frequency, onset, and duration of EVD clinical signs and symptoms were performed during the 1995 outbreak in Kikwit, Zaire (EBOV) and the 2007–2008 outbreak in Bundibugyo, Uganda (BDBV). The mean incubation period, best calculated currently for EVD outbreaks due to EBOV infection, is 12.7 days (standard deviation = 4.3 days), but can be as long as 25 days. EVD begins with a sudden onset of an influenza-like stage characterized by general malaise, fever with chills, arthralgia and myalgia, and chest pain. Nausea is accompanied by abdominal pain, anorexia, diarrhea, and vomiting. Respiratory tract involvement is characterized by pharyngitis with sore throat, cough, dyspnea, and hiccups. The central nervous system is affected as judged by the development of severe headaches, agitation, confusion, fatigue, depression, seizures, and sometimes coma.
Cutaneous presentation may include: maculopapular rash, petechiae, purpura, ecchymoses, and hematomas (especially around needle injection sites). Development of hemorrhagic symptoms is generally indicative of a negative prognosis. However, contrary to popular belief, hemorrhage does not lead to hypovolemia and is not the cause of death (total blood loss is low except during labor). Instead, death occurs due to multiple organ dysfunction syndrome (MODS) due to fluid redistribution, hypotension, disseminated intravascular coagulation, and focal tissue necroses.
Treatment:
There is currently no FDA-approved ebolavirus-specific therapy for EVD. Treatment is primarily supportive in nature and includes minimizing invasive procedures, balancing fluids and electrolytes to counter dehydration, administration of anticoagulants early in infection to prevent or control disseminated intravascular coagulation, administration of procoagulants late in infection to control hemorrhaging, maintaining oxygen levels, pain management, and administration of antibiotics or antimycotics to treat secondary infections. Hyperimmune equine immunoglobulin raised against EBOV has been used in Russia to treat a laboratory worker who accidentally infected herself with EBOV—but the patient died anyway. Experimentally, recombinant vesicular stomatitis Indiana virus (VSIV) expressing the glycoprotein of EBOV or SUDV has been used successfully in nonhuman primate models as post-exposure prophylaxis. Such a recombinant post-exposure vaccine was also used to treat a German researcher who accidentally pricked herself with a possibly EBOV-contaminated needle. Treatment might have been successful as she survived. However, actual EBOV infection could never be demonstrated without a doubt. Novel, very promising, experimental therapeutic regimens rely on antisense technology. Both small interfering RNAs (siRNAs) and phosphorodiamidate morpholino oligomers (PMOs) targeting the EBOV genome could prevent disease in nonhuman primates.
Referal sources and evidences of this disease:
The above video is about ebola virus outbreak .
Case studies
Unrecognized Ebola Hemorrhagic Fever at
Mosango Hospital during the 1995
Epidemic in Kikwit, Democratic Republic
of the Congo:
On April 20, 1995, a 70-year-old nun, working
as a nurse in Kikwit General Hospital, was
admitted to Mosango General Hospital with a 5-
day history of fever, despite antimalarial
treatment. The day before hospitalization she
had profuse diarrhea, vomiting, high fever, and
severe agitation with delirium. On arrival, quiet
and apyretic, she complained of headache, loss of
appetite, and severe asthenia, but she walked to
her room without help. On examination, the only
abnormalities recorded were severe dehydration
and oral thrush-like lesions, raising a suspicion of
candidiasis. Pulse rate was 80/min and blood
pressure 120/80. Medical history included an
amebiasis liver abscess 15 years ago and chronic
coronaritis since 1990.
Electrocardiogram (ECG) abnormalities were
consistent with chronic diffuse ischemia. Laboratory
investigations showed the following values:
few trophozoites on a thick film; erythrocyte
sedimentation rate (ESR) 15 mm/h; bleeding time
(BT) 7½ min; coagulation time (CT) 9 min; and
white blood cells (WBC) 8.4x10
9/L (73% neutrophils,
23% lymphocytes, 2% eosinophils, 1%
basophils, 1% mastocytes). Urinalysis showed
proteinuria (++), hyaline cylinders (+++), 50
white cells per field, and hematuria (+). The
patient was perfused with 4L/day of glucose and
1.5 g of quinine. She was kept in a private room in
the nearby nuns’ convent.
Later during the day, high fever (40°C) and
severe diarrhea with melena developed; the pulse
rate was normal (80/min). Typhoid fever was
suspected despite the lack of hepatosplenomegaly;
Widal test was not available for
confirmation. Treatment was started with
intravenous (i.v.) amoxicillin (1g/6h during the
first 24 h and then 1g/4h) and i.v. chloramphenicol
bleeding cracks on the lips and diffuse bleeding in
the oral cavity (i.e., gums, tongue). The volume of
urine was low, and antibiotic therapy was
changed to cephalosporin.
On hospitalization day 5, hemorrhages increased,
and fever remained high until the end of
the day, when it started to normalize. Urine volume
was still low (verified by vesical catheter) despite
the i.v. rehydration of 4 L/day. Fresh blood
transfusion (300 ml) did not slow the hemorrhaging;
disseminated intravascular coagulation was
suspected, and heparin treatment was started.
The patient became comatose. The laboratory
results showed ESR 55mm/h and WBC 30.2x10
9/
L with an unchanged formula. No coagulation
was observed on BT and CT. Blood pressure fell
(80/50); the clinical status remained unchanged
until the patient’s death on April 25 at 10:00 a.m.
No special nursing precautions were taken
either during the hospitalization or after the
death, and the body was transferred to Kikwit to
be buried. On April 30, another nun who took care of
the index patient during the night of April 23
became ill with fever, headache, and myalgia. Over
the next few days, the second patient had a clinical
picture identical to that of the index patient,
including high fever, severe asthenia, vomiting,
hiccups, and diarrhea. On May 5, epistaxis and
coagulation abnormalities developed, followed by
other clinical signs of the hemorrhagic syndrome.
The second patient was transferred to Kikwit
General Hospital, where she died 6 days later. A
laboratory confirmation of Ebola hemorrhagic fever
was made on a blood specimen collected on May 5
and sent to Special Pathogens Branch (Centers for
Disease Control and Prevention, Atlanta, GA).
These cases of unrecognized Ebola hemorrhagic
fever were part of the hospital outbreak
that precipitated and mobilized international
community efforts (2). Retrospectively, the
clinical symptoms observed were typical of Ebola
hemorrhagic fever (3,4) and were described again
in subsequent patients during this outbreak (5).
In tropical Africa, the presence of hemorrhagic
symptoms in the course of a febrile illness should
raise the possibility of one of the viral hemorrhagic
fever diseases. In viral hemorrhagic fevers,
maculopapular rash is constantly observed only in
filovirus disease. Typically, the clinical laboratory
findings include an early lymphopenia and marked
thrombocytopenia. Containment and barrier nursing
procedures should be initiated until the
diagnosis of viral hemorrhagic fever can be ruled
out. The index patient described here was the third
patient transferred from Kikwit General Hospital
in less than 1 month to die of a hemorrhagic
illness after a few days of an unexplained febrile
syndrome. Two patients were health-care
workers in Kikwit General Hospital. This cluster
of hemorrhagic illness and possible human-tohuman
transmission, particularly among hospital
staff, was (and should always be) sufficient to
suspect a viral hemorrhagic fever. The laboratory
confirmation of this presumptive diagnosis was
the clenching factor in
he multinational effort in
Kikwit.
Virology
Main article: Ebola virus
Genome
Electron micrograph of an Ebola virus virion
Like all mononegaviruses, ebolavirions contain linear nonsegmented, single-stranded, non-infectious RNAgenomes of negative polarity that possesses inverse-complementary 3' and 5' termini, do not possess a 5' cap, are not polyadenylated, and are not covalently linked to a protein. Ebolavirus genomes are approximately 19 kilobase pairs long and contain seven genes in the order 3'-UTR-NP-VP35-VP40-GP-VP30-VP24-L-5'-UTR.The genomes of the five different ebolaviruses (BDBV, EBOV, RESTV, SUDV, and TAFV) differ in sequence and the number and location of gene overlaps.
Structure
Like all filoviruses, ebolavirions are filamentous particles that may appear in the shape of a shepherd's crook or in the shape of a "U" or a "6", and they may be coiled, toroid, or branched. Ebolavirions are generally 80 nm in width, but vary somewhat in length. In general, the median particle length of ebolaviruses ranges from 974–1,086 nm (in contrast to marburgvirions, whose median particle length was measured to be 795–828 nm), but particles as long as 14,000 nm have been detected in tissue culture. Ebolavirions consist of seven structural proteins. At the center is the helicalribonucleocapsid, which consists of the genomic RNA wrapped around a polymer of nucleoproteins (NP). Associated with the ribonucleoprotein is the RNA-dependent RNA polymerase (L) with the polymerase cofactor (VP35) and a transcription activator (VP30). The ribonucleoprotein is embedded in a matrix, formed by the major (VP40) and minor (VP24) matrix proteins. These particles are surrounded by a lipid membrane derived from the host cell membrane. The membrane anchors a glycoprotein (GP) that projects 7 to 10 nm spikes away from its surface. While nearly identical to marburgvirions in structure, ebolavirions are antigenically distinct.
Replication
The ebolavirus life cycle begins with virion attachment to specific cell-surface receptors, followed by fusion of the virion envelope with cellular membranes and the concomitant release of the virus nucleocapsid into the cytosol. The viral RNA polymerase, encoded by the L gene, partially uncoats the nucleocapsid and transcribes the genes into positive-stranded mRNAs, which are then translated into structural and nonstructural proteins. Ebolavirus RNA polymerase (L) binds to a single promoter located at the 3' end of the genome. Transcription either terminates after a gene or continues to the next gene downstream. This means that genes close to the 3' end of the genome are transcribed in the greatest abundance, whereas those toward the 5' end are least likely to be transcribed. The gene order is therefore a simple but effective form of transcriptional regulation. The most abundant protein produced is the nucleoprotein, whose concentration in the cell determines when L switches from gene transcription to genome replication. Replication results in full-length, positive-stranded antigenomes that are in turn transcribed into negative-stranded virus progeny genome copy. Newly synthesized structural proteins and genomes self-assemble and accumulate near the inside of the cell membrane. Virions bud off from the cell, gaining their envelopes from the cellular membrane they bud from. The mature progeny particles then infect other cells to repeat the cycle.
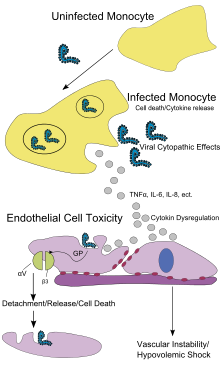
Pathophysiology
Pathogenesis schematic
Endothelial cells, mononuclear phagocyte, and hepatocytes are the main targets of infection. After infection, in a secreted glycoprotein (sGP) the Ebola virus glycoprotein (GP) is synthesized. Ebola replication overwhelms protein synthesis of infected cells and host immune defenses. The GP forms a trimeric complex, which binds the virus to the endothelial cells lining the interior surface of blood vessels. The sGP forms a dimeric protein which interferes with the signaling of neutrophils, a type of white blood cell, which allows the virus to evade the immune system by inhibiting early steps of neutrophil activation. These white blood cells also serve as carriers to transport the virus throughout the entire body to places such as the lymph nodes, liver, lungs, and spleen. The presence of viral particles and cell damage resulting from budding causes the release of cytokines (specifically TNF-α, IL-6, IL-8, etc.), which are the signaling molecules for fever and inflammation. The cytopathic effect, from infection in the endothelial cells, results in a loss of vascular integrity. This loss in vascular integrity is furthered with synthesis of GP, which reduces specific integrins responsible for cell adhesion to the inter-cellular structure, and damage to the liver, which leads to coagulopathy.
Diagnosis
EVD is clinically indistinguishable from Marburg virus disease (MVD), and it can also easily be confused with many other diseases prevalent in Equatorial Africa, such as other viral hemorrhagic fevers, falciparum malaria, typhoid fever, shigellosis, rickettsial diseases such as typhus, cholera, gram-negativesepticemia, borreliosis such as relapsing fever or EHEC enteritis. Other infectious diseases that ought to be included in the differential diagnosis include leptospirosis, scrub typhus, plague, Q fever, candidiasis, histoplasmosis, trypanosomiasis, visceralleishmaniasis, hemorrhagic smallpox, measles, and fulminant viral hepatitis. Non-infectious diseases that can be confused with EVD are acute promyelocytic leukemia, hemolytic uremic syndrome, snakeenvenomation, clotting factor deficiencies/platelet disorders, thrombotic thrombocytopenic purpura, hereditary hemorrhagic telangiectasia, Kawasaki disease, and even warfarin intoxication.
The most important indicator that may lead to the suspicion of EVD at clinical examination is the medical history of the patient, in particular the travel and occupational history (which countries were visited?) and the patient's exposure to wildlife (exposure to bats, bat excrement, nonhuman primates?). EVD can be confirmed by isolation of ebolaviruses from or by detection of ebolavirus antigen or genomic or subgenomic RNAs in patient blood or serum samples during the acute phase of EVD. Ebolavirus isolation is usually performed by inoculation of grivet kidney epithelial Vero E6 or MA-104 cell cultures or by inoculation of human adrenal carcinoma SW-13 cells, all of which react to infection with characteristic cytopathic effects. Filovirions can easily be visualized and identified in cell culture by electron microscopy due to their unique filamentous shapes, but electron microscopy cannot differentiate the various filoviruses alone despite some overall length differences.Immunofluorescence assays are used to confirm ebolavirus presence in cell cultures. During an outbreak, virus isolation and electron microscopy are most often not feasible options. The most common diagnostic methods are therefore RT-PCR in conjunction with antigen-capture ELISA which can be performed in field or mobile hospitals and laboratories. Indirect immunofluorescence assays (IFAs) are not used for diagnosis of EVD in the field anymore.
Prevention
A researcher working with the Ebola virus while wearing a BSL-4 positive pressure suit to avoid infection
Ebola viruses are highly infectious as well as contagious.
As an outbreak of ebola progresses, bodily fluids from diarrhea, vomiting, and bleeding represent a hazard. Due to lack of proper equipment and hygienic practices, large-scale epidemics occur mostly in poor, isolated areas without modern hospitals or well-educated medical staff. Many areas where the infectious reservoir exists have just these characteristics. In such environments, all that can be done is to immediately cease all needle-sharing or use without adequate sterilization procedures, isolate patients, and observe strict barrier nursing procedures with the use of a medical-rated disposable face mask, gloves, goggles, and a gown at all times, strictly enforced for all medical personnel and visitors. The aim of all of these techniques is to avoid any person’s contact with the blood or secretions of any patient, including those who are deceased.
Vaccines have successfully protected nonhuman primates; however, the six months needed to complete immunization made it impractical in an epidemic. To resolve this, in 2003, a vaccine using an adenoviral (ADV) vector carrying the Ebola spike protein was tested on crab-eating macaques. The monkeys were challenged with the virus 28 days later, and remained resistant.In 2005, a vaccine based on attenuated recombinant vesicular stomatitis virus (VSV) vector carrying either the Ebola glycoprotein or Marburg glycoprotein successfully protected nonhuman primates, opening clinical trials in humans. By October, the study completed the first human trial; giving three vaccinations over three months showing capability of safely inducing an immune response. Individuals were followed for a year, and, in 2006, a study testing a faster-acting, single-shot vaccine began. This study was completed in 2008. The next step is to try the vaccine on a strain of Ebola that is closer to the one that infects humans.
There are currently no Food and Drug Administration-approved vaccines for the prevention of EVD. Many candidate vaccines have been developed and tested in various animal models. Of those, the most promising ones are DNA vaccines or are based on adenoviruses,vesicular stomatitis Indiana virus (VSIV)or filovirus-like particles (VLPs) as all of these candidates could protect nonhuman primates from ebolavirus-induced disease. DNA vaccines, adenovirus-based vaccines, and VSIV-based vaccines have entered clinical trials.
Contrary to popular belief, ebolaviruses are not transmitted by aerosol during natural EVD outbreaks. Due to the absence of an approved vaccine, prevention of EVD therefore relies predominantly on behavior modification, proper personal protective equipment, and sterilization/disinfection.
On 6 December 2011, the development of a successful vaccine against Ebola for mice was reported. Unlike the predecessors, it can be freeze-dried and thus stored for long periods in wait for an outbreak. The research will be presented in Proceedings of National Academy of Sciences.
In endemic zones
The natural maintenance hosts of ebolaviruses remain to be identified. This means that primary infection cannot necessarily be prevented in nature. The avoidance of EVD risk factors, such as contact with nonhuman primates or bats, is highly recommended, but may not be possible for inhabitants of tropical forests or people dependent on nonhuman primates as a food source.
During outbreaks
Since ebola viruses do not spread via aerosol, the most straightforward prevention method during EVD outbreaks is to avoid direct (skin-to-skin) contact with patients, their excretions and body fluids, or possibly contaminated materials and utensils. Patients should be isolated and medical staff should be trained and apply strict barrier nursing techniques (disposable face mask, gloves, goggles, and a gown at all times). Traditional burial rituals, especially those requiring embalming of bodies, should be discouraged or modified, ideally with the help of local traditional healers.
In the laboratory
Ebolaviruses are World Health Organization Risk Group 4 Pathogens, requiring Biosafety Level 4-equivalent containment. Laboratory researchers have to be properly trained in BSL-4 practices and wear proper personal protective equipment.
Why is this troublesome? The most significant and alarming consequence of early maturation is an increased risk for breast cancer in adulthood. Early menarche is an established risk factor for breast cancer, and this is believed to be due to the extended lifetime exposure to ovarian hormones. Similarly, exposure to EDCs during childhood is associated with hormonal cancers, such as breast and testicular cancers.
Girls of 7, 8 or 9 years old are not emotionally or psychologically equipped to handle puberty. As such, earlier puberty is also associated with a higher risk of psychological problems during adolescence such as anxiety, depression, and eating disorders. Girls who mature earlier are also more likely to take part in risky behaviors like smoking and alcohol use.
Oxytocin is a hormone secreted by the pituitary gland. It is naturally produced in an expectant mother for two purposes. On one hand it promotes lactation, while it helps in contracting the uterine muscles after child birth to check loss of blood. It was artificially manufactured to save mothers from post-pregnancy complications. A section of scientific literature says that children born to mothers exposed to high level of artificial oxytocin may suffer with birth defects and low resistance levels. In individual cases, oxytocin is said to have inhibited breast feeding.
Certain experts however refute the claims. It is said that oxytocin was a protein that was naturally flushed out of the body if taken through the oral route. "Since oxytocin doesn't absorb through the oral route it is always given through intra venous or nasal route," . "The good and bad effect of oxytocin on humans administered through the oral route is being debated world over," .Artificial oxytocin was placed in Schedule H of the Drug and Cosmetics Act and can be sold on prescription only. It was banned in India for use on animals. Though the price of generic oxytocin being manufactured and marketed by reputed companies is around Rs 20, it is claimed to be readily available in black - the cost of a single ampoule being less than a rupee. "No matter how illiterate the milk man is, he knows what oxytocin is," remarked an animal activist. Also, oxytocin being used by certain milk men is different from what pharma companies manufacture commercially. "Dairymen cannot use the normal oxytocin as it is available only on prescription basis. So they bank on illegal source. And one has all the reasons to doubt if they were manufactured correctly or not," said a government veterinary officer.
In cows or buffaloes, the flow of milk is stimulated by the calf's nuzzling, since dairy men kill the calf or else separate it from the mother, they inject the cow with oxytocin to stimulate uterine contractions and allow for easy flow of milk. Veterinary experts revealed that oxytocin was a slow poison for the bovine. "Oxytocin does not increase the amount of milk but merely makes it flow faster. It causes the equivalent of labor pains in the cow twice a day and destroys her reproductive system prematurely. She grows sterile in four years and is then abandoned onto the street or else slaughtered."
Oxytocin in a nine amino acid peptide that is synthesized in hypothalamic neurons and transported down axons of the posterior pituitary for secretion into blood. Oxytocin is also secreted within the brain and from a few other tissues, including the ovaries and testes. Oxytocin differs from antidiuretic hormone in two of the nine amino acids. Both hormones are packaged into granules and secreted along with carrier proteins called neurophysins.
Physiologic Effects of Oxytocin
In old days, oxytocin had the reputation of being an "uncomplicated" hormone, with only a few well-defined activities related to birth and lactation. As has been the case with so many hormones, further research has demonstrated many subtle but profound influences of this little peptide. For example, administration of oxytocin to species ranging from mice to humans has revealed a number of effects on social behavior. Nevertheless, it has been best studied in females where it clearly mediates three major effects:
1. Stimulation of milk ejection (milk letdown): Milk is initially secreted into small sacs within the mammary gland called alveoli, from which it must be ejected for consumption or harvesting. Mammary alveoli are surrounded by smooth muscle (myoepithelial) cells which are a prominant target cell for oxytocin. Oxytocin stimulates contraction of myoepithelial cells, causing milk to be ejected into the ducts and cisterns.
2. Stimulation of uterine smooth muscle contraction at birth: At the end of gestation, the uterus must contract vigorously and for a prolonged period of time in order to deliver the fetus. During the later stages of gestation, there is an increase in abundance of oxytocin receptors on uterine smooth muscle cells, which is associated with increased "irritability" of the uterus (and sometimes the mother as well). Oxytocin is released during labor when the fetus stimulates the cervix and vagina, and it enhances contraction of uterine smooth muscle to facilitate parturition or birth.
In cases where uterine contractions are not sufficient to complete delivery, physicians and veterinarians sometimes administer oxytocin ("pitocin") to further stimulate uterine contractions - great care must be exercised in such situations to assure that the fetus can indeed be delivered and to avoid rupture of the uterus.
Establishment of maternal behavior: Successful reproduction in mammals demands that mothers become attached to and nourish their offspring immediately after birth. It is also important that non-lactating females do not manifest such nurturing behavior. The same events that affect the uterus and mammary gland at the time of birth also affect the brain. During parturition, there is an increase in concentration of oxytocin in cerebrospinal fluid, and oxytocin acting within the brain plays a major role in establishing maternal behavior.
Evidence for this role of oxytocin comes from two types of experiments. First, infusion of oxytocin into the ventricles of the brain of virgin rats or non-pregnant sheep rapidly induces maternal behavior. Second, administration into the brain of antibodies that neutralize oxytocin or of oxytocin antagonists will prevent mother rats from accepting their pups. Other studies support the contention that this behavioral effect of oxytocin is broadly applicable among mammals.
Use/Abuse of Oxytocin in Pakistan
Dairy farming today in Pakistan has changed a lot. Milkmen demand timed delivery and so do the consumers. For example, I need my morning tea at 7am so my milk should arive by 6am in the morning. I return from my office by 7pm, on my way back home I buy milk lets say 6:45pm, so I demand the milk should be available by that time. On the other hand a cow's lactacting system depends on the need of the calf not me! Human is the only mammal who drinks milk even after weaning. From farm to local retailer it takes a lot of time, just to sychronize everything -- from milking to selling. We now have synchronized milking. Need milk? Inject 2cc oxytocin and cow is ready for milking within minutes. Oxytocin is the most wildly producing and selling hormone across Pakistan.
Side effects of Artificially Induced Oxytocin
Each time a cow is given oxytocin she passes urine (due to labour pain) and all of the artificially induced oxytocin is removed from the body. There have been so many lab tests done, but those lab-men never found no signs of it. Which means oxytocin is not bad for human health, but. There is always a but! Each shot of oxytocin stimulates contraction of myoepithelial cells and it enhances contraction of uterine smooth muscle. This differs from the natural secretion of oxytocin released within the body. Thus giving a cow labour pain again and again. This synchronous urethral stimulation makes a cow sterile, means which won't be able to give birth ever.
Major side effect is that cows of better quality go to slaughterhouse right after their first lactation. Pakistan is losing it best milk producing breeds of both; cows and buffalos. No commercial farmer is willing to stop abusing artificial oxytocin to his dairy herd. Today our cows are just like a milk dispencer, give 'em a shot of 'tocin and fill your jug of milk!
A technique developed by Johns Hopkins surgeons is providing a new route to get to and remove tumors buried at the base of the skull: through the natural hole behind the molars, above the jawbone and beneath the cheekbone.
In a report detailing the novel surgery, published in the October 2011 issue of The Laryngoscope, the surgeons say the procedure, already performed in seven patients, yields faster recovery and fewer complications than traditional approaches. And, because the incisions are made inside the cheek, there are no visible scars.
Kofi Boahene, M.D., an assistant professor of facial plastic and reconstructive surgery and otolaryngology-head and neck surgery at the Johns Hopkins University School of Medicine, says the idea for the new approach came to him when a 20-year-old female patient previously treated for a brain tumor developed a new tumor deep in the skull base.
Traditional surgeries to remove skull base tumors require incisions through the face and bone removal, which can sometimes be disfiguring. Additionally, these operations can harm facial nerves, leading to paralysis that affects facial expressions and days or weeks of hospitalization and recovery. Boahene said he was gazing at a skull model in his office, considering options to spare his patient from another traditional surgery. "I looked at the 'window" that already exists in the skull, above the jawbone and below the cheekbone and realized this was an access route not previously recognized for this kind of surgery," he said.
Knowing there was always the option of switching to the traditional approach while trying the new approach, Boahene and his colleagues performed the new procedure on his patient last year. The expected surgery time shrunk from six hours to two. Additionally, the patient was able to leave the hospital the next day and return to college, with no visible evidence that she had surgery performed.
The report in The Laryngoscope describes details of the surgeries on three of the seven patients Boahene and his colleagues have thus far treated. Besides benefits for patients, he and his colleagues note, the new procedure is significantly less complicated for surgeons to perform, provides excellent visualization of the skull base area, and could potentially save health care dollars due to patients' shorter hospital stays.
Not all patients are candidates for this procedure, Boahene cautions. It isn't an option for those with very large skull base tumors or those with tumors that wrap around blood vessels. For these patients, traditional skull base surgery is still the best choice, he says.
In the future, he and his colleagues plan to try the new procedure using a surgical robot, which could provide even better visualization for surgeons and further reduce chances of complications for patients.
One subtype of breast cancer shares many genetic features with high-grade serous ovarian cancer, a cancer that is very difficult to treat, according to researchers supported by the National Institutes of Health. The findings suggest that the two cancers are of similar molecular origin, which may facilitate the comparison of therapeutic data for subtypes of breast and ovarian cancers.
The researchers, using data generated as part of The Cancer Genome Atlas (TCGA), described new insights into the four standard molecular subtypes based on a comprehensive characterization of samples from 825 breast cancer patients.
The study, a collaborative effort funded by the National Cancer Institute (NCI) and the National Human Genome Research Institute (NHGRI), both part of NIH, was published online Sept. 23, 2012, and in print Oct. 4, 2012, in the journal Nature.
“TCGA’s comprehensive characterization of their high-quality samples allows researchers an unprecedented look at these breast cancer subgroups,” said NIH Director Francis S. Collins, M.D., Ph.D.
Breast cancer cells seen under the microscope, with the HER2 protein, which can trigger cell growth responses, lit up in bright red
Analyses of genomic data have confirmed that there are four primary subtypes of breast cancer, each with its own biology and survival outlooks. These TCGA findings are based on a large number of breast cancer specimens that capture a complete view of the genomic alterations. The four groups are called intrinsic subtypes of breast cancer: HER2-enriched (HER2E), Luminal A (LumA), Luminal B (LumB) and Basal-like. A fifth type, called Normal-like, was observed, but because of small numbers (only eight specimens) the researchers were unable to rigorously study it.
The TCGA Research Network uncovered marked genomic similarities between the Basal-like subtype and serous ovarian cancer. The mutation spectrum, or types and frequencies of genomic mutations, were largely the same in both cancer types. Further analyses identified several additional common genomic features, such as gene mutation frequency, suggesting that diverse genomic aberrations can converge into a limited number of cancer subtypes.
Computational analyses show that Basal-like breast cancer and serous ovarian cancer might both be susceptible to agents that inhibit blood vessel growth, cutting off the blood supply to the tumor, as well as to compounds that target DNA repair, which include chemotherapy drugs such as cisplatin.
The Basal-like subgroup has also been called Triple Negative Breast Cancer because many, though not all, Basal-like tumors are negative when tested for three receptors: the estrogen receptor, the progesterone receptor and human epidermal growth factor receptor 2 (HER2). These receptors can trigger potent cell growth responses and act like a nametag, identifying the cell to the environment. The absence of these receptors means that treatments that target them will most likely be ineffective.
“The molecular similarity of one of the principal subtypes of breast cancer to that found in ovarian cancer gives us additional leverage to compare treatments and outcomes across these two cancers,” noted Harold Varmus, M.D., NCI director. “This treasure trove of genetic information will need to be examined in great detail to identify how we can use it functionally and clinically.”
According to the World Health Organization, there are approximately 1.3 million new cases of breast cancer and 450,000 deaths worldwide annually. Breast cancer is the most common cancer among women. The majority of cases are sporadic, meaning there is not a family history of breast cancer, as opposed to genetic, where genes predispose a person to the disease. Men can also develop breast cancer, but it accounts for less than 1 percent of breast cancer cases.
Breast cancer tumors that have the HER2 receptor are called HER2-positive, and those that don't are called HER2-negative. When researchers analyzed the genomic findings from tumors determined to be HER2-positive by standard cellular tests, they found that only half of the samples could be characterized as belonging to the HER2E subtype. The other half were characterized as Luminal subtypes, suggesting that there are at least two types of clinically defined HER2-positive tumors.
In general, the Luminal subtypes had the lowest overall mutation rate, but by contrast, had the largest number of genes observed to be significantly mutated. This suggests that each of the genes identified as significantly mutated in the Luminal subtypes is more likely to be important in fueling cancer progression. The Luminal subtypes are characterized by the specific expression signature of multiple so-called transcription-factor genes, including ESR1, GATA3, FOXA1, XBP1 and cMYB. These genes have a complex interaction, cooperating in an orchestrated series of activations. GATA3 and FOXA1 are frequently mutated, but those mutations are mutually exclusive, meaning that mutations were observed in either GATA3 or FOXA1 but never in both. However, ERS1 and XBP1 are highly expressed but infrequently mutated.
The scale of the TCGA program allows researchers to perform the integrative analyses that detect these complex patterns of genomic changes and interactions. This close inspection of the cancer genome has led to a deeper understanding of the mutations essential for cancer progression, and several new candidates were identified in this study. The authors hope that discovery of these mutations will be a crucial step toward improving breast cancer therapies.
This publication focuses on the discoveries made through a combined analysis involving data from 825 breast cancer cases, which are freely available in the TCGA Data Portal, with several hundred more cases to come.
“The data generated by the TCGA program comprise a vast resource that investigators will be analyzing for years to come. The resource of information about breast cancer genomes will undoubtedly fuel myriad discoveries by the cancer research community,” said Eric D. Green, M.D., Ph.D., NHGRI director.
So far, The Cancer Genome Atlas Research Network has published analyses on these cancers: • glioblastoma multiforme (http://cancergenome.nih.gov/newsevents/newsannouncements/news_9_4_2008) • ovarian serous adenocarcinoma (http://cancergenome.nih.gov/newsevents/newsannouncements/ovarianpaper) • colorectal adenocarcinoma (http://www.cancer.gov/newscenter/newsfromnci/2012/TCGAcolorectal) • lung squamous cell carcinoma (http://www.cancer.gov/newscenter/newsfromnci/2012/LungSquamousTCGA)
Did any one ever think that "a sexual enhancer" can be a life saving drug for some one?
Few facts about Viagra:
Sildefanil was synthesized by a group of pharmaceutical chemists at Pfizers' research facility in England. It was initially studied for use in hypertension and angina.
Phase I clinical trials suggested that the drug had little effect on angina, but that it could induce marked penile erections. Pfizer therefore decided to market it for erectile dysfunction, rather than for angina. The drug was patented in 1996, approved for use in erectile dysfunction by the US FDA on March 27, 1998, becoming the first oral treatment approved to treat erectile dysfunction in the United States.
Oral Sildenafil in Infants With Persistent Pulmonary Hypertension of the Newborn:
•Persistent pulmonary hypertension (PPHN) occurs in as many as 6.8 of 1000 live births.
•Mortality is ∼10% to 20% with high-frequency ventilation,
•Sildenafil is a phospho diesterase inhibitor type 5 that selectively reduces pulmonary vascular resistance.
Treatment of Severe Altitude Sickness using Viagra:
•High altitude can sometimes cause illness, especially in people with existing heart and lung problems. The thinner air or lack of oxygen at higher altitudes can cause blood vessels to constrict. When this occurs within the lungs, the constriction of blood vessels can put more force on the heart, leading to life-threatening heart failure.
•High-altitude pulmonary edema (HAPE) occurs when high altitude and low air pressure causes fluid to leak from blood vessels and builds up in the lungs, interfering with oxygen exchange.. HAPE has a mortality rate of 44% if untreated. It's triggered by intense physical exertion at high altitudes that people aren't accustomed to.
•Viagra works by relaxing blood vessels, allowing more blood to flow freely through vessels. The researchers used this drug to block the effects of high altitude on blood vessels on the lung.
Sildenafil in the treatment of pulmonary arterial Hypertension:
•Pulmonary arterial hypertension (PAH) is a progressive, and often fatal, debilitating disorder. The clinical hallmarks of this disease include: 1) progressive breathlessness 2) exertion limitation and 3) frequent decline and failure of the right ventricle.
•The increased pulmonary artery pressure found in PAH is due to disturbances in key vascular mediator pathways including relative deficiencies of vasodilators
•Sildenafil is a selective Phosphodiesterase-5 inhibitor that has been reported to be a potent pulmonary vasodilator. Sildenafil selectively inhibits phosphodiesterase 5 (PDE5 is abundant in pulmonary and penile tissue) which leads to stabilization of cyclic guanosine monophosphate (cGMP). cGMP is a second messenger of nitric oxide (NO). Stabilization of cGMP results in increasing nitric oxide (NO) at the tissue level leading to pulmonary vessel vasodilatation.
•Sildenafil administered orally has been shown to have beneficial effects in patients with PAH.
On a whole the viagra(Sildefanil) is found to be a potent life saver in many aspects and doctors found it to be a very attractive drug for cardiac conditions and lowering blood pressure and noticed that when they prescribe Viagra to patients with a heart condition it actually improves their heart condition as well as their erectile dysfunction.
•The problem doctors see in premature babies with breathing difficulties is - although oxygen can be blown into their lungs to help them, there isn't enough blood supply to various areas of the lungs to take the oxygen around the rest of the body. What Sildenafil does is open up the blood vessels so they can capture the oxygen and take it around the body
Thus Sildenafil or Viagra as it is popularly known world over, has shown multi faceted personality over the years and helped the medical community in combating severe diseases and ailments.As time passes, research may unfold cures to many more ailments through the use of Viagra.